Introduction
Gas bubble disease (GBD) is a condition in which free gas bubbles form in the blood and tissues of fish. It leads to impaired microcirculation, gill damage, organ destruction, and in some cases, death.
A common explanation — “air bubbles entered the gills and blocked them” — is incorrect. It replaces the actual mechanism and prevents proper interpretation of both clinical signs and necropsy findings.
A detailed explanation of the mechanism is provided
here
 Gas Bubble Disease: It's Not About the Bubbles
Gas Bubble Disease in fish is not caused by air bubbles entering the gills but by dissolved gas supersaturation. This article explains the …
.
Gas Bubble Disease: It's Not About the Bubbles
Gas Bubble Disease in fish is not caused by air bubbles entering the gills but by dissolved gas supersaturation. This article explains the …
.
Why diagnosis is difficult
Gas bubble disease does not always produce obvious signs: bubbles may be absent, disappear after death, be sparse, or have no diagnostic value, as noted in broader analyses of gas bubble trauma in fish (Pleizier et al., 2020).
Acute cases with clearly visible bubbles are the exception rather than the rule.
In most situations, the process is chronic and subtle, remaining unnoticed externally.
Where the problem originates
In systems with pumps, pressure often exceeds atmospheric levels. This increases gas solubility in water. If air is entrained at the pump intake, or if cavitation or microbubbles are present, a gas–water mixture is formed.
This results in gas supersaturation, which in closed aquatic systems is considered one of the key drivers of gas bubble disease (Hong et al., 2024).
In acute cases, this may lead to rapid mortality with obvious signs:
- gas in the eyes
- bubbles in fins
- gas accumulation in body cavities
However, this is not the typical scenario.
What actually happens
Under chronic supersaturation, gas exchange becomes impaired. Oxygen may still enter tissues, but inert gases (primarily nitrogen) are not effectively eliminated. They accumulate in dissolved form (Pleizier et al., 2020).
This leads to:
- microcirculatory disruption
- blood stasis
- development of ischemia followed by tissue hypoxia
Despite the presence of blood in the organs, it does not perform its function.
The presence of blood in a tissue does not indicate effective circulation.
What this leads to
With prolonged exposure, a sequential cascade develops:
- impaired gas exchange
- microcirculatory disturbances
- ischemia
- hypoxia
- tissue destruction
The most sensitive organs are:
- gills
- kidney
- brain
These are the structures most commonly affected during necropsy.
Ischemia is a condition in which tissue experiences oxygen deficiency due to impaired blood supply or microcirculation.
Important
The presence of gas in tissues at necropsy is not, by itself, evidence of gas bubble disease.
Postmortem gas bubbles may form due to:
- warming of the body
- autolysis
- pressure changes
This is especially noticeable when fish are kept in cold water but examined at higher temperatures. As temperature increases, gas solubility decreases, and dissolved gases come out of solution, forming bubbles.
Thus, the presence of gas at necropsy reflects not only processes that occurred during life, but also changes that develop after death.
Context is more important than individual findings.
Consequences. Macro- and microscopic picture
The fish heart pumps venous blood. Circulation is single-loop: blood passes through the gills for gas exchange, then distributes to tissues and returns to the heart.
The heart directs blood flow toward the head. Because vessels are located close to the surface in the rostral region, circulatory disturbances may become visually apparent.
Blood stasis is associated with:
- redness
- vascular engorgement
- dilation
- hyperemia

Necrosis is cell death occurring during life.
Degeneration refers to tissue breakdown after death.

Microcirculatory disturbances lead to venous congestion, increased pressure, and vascular damage. These changes reflect the development of ischemia in nervous tissue.
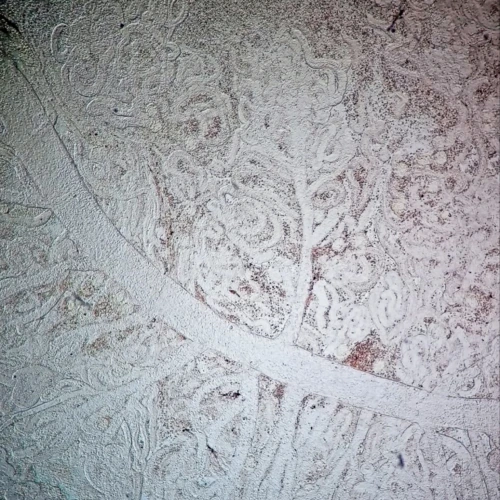
The kidney in fish consists of head and trunk regions.
The trunk kidney lies along the позвоночник beneath the swim bladder and contains renal tubules — the main functional structures. A large volume of blood passes through it, so microcirculatory disturbances quickly lead to pronounced changes.
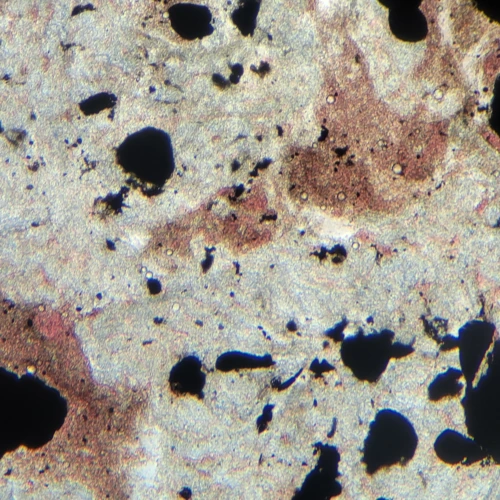
Typical findings include:
- hyperemia
- tubular destruction
- tissue necrosis
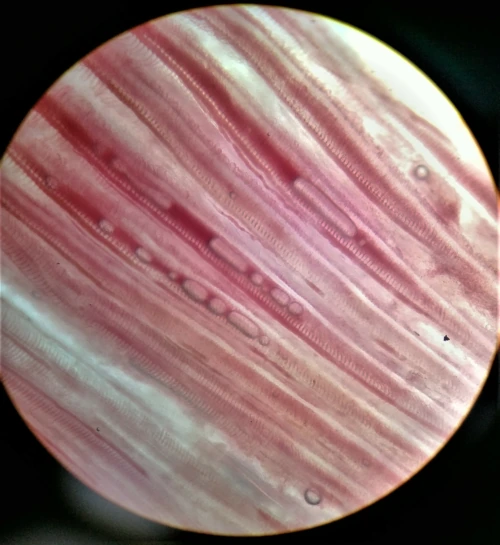
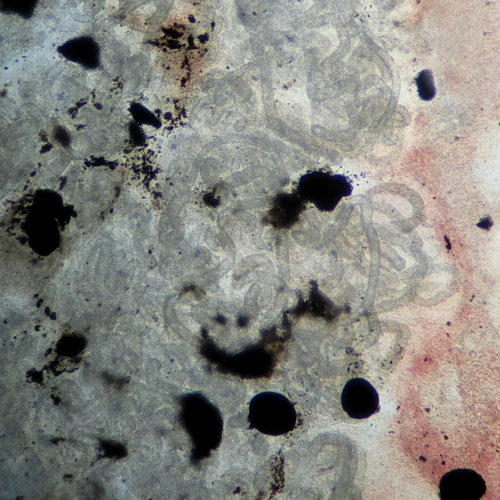
The image shows a compression preparation of the trunk (posterior) kidney of a fish. In contrast to the head kidney, which primarily performs hematopoietic and immune functions and is composed of loose hematopoietic tissue, the trunk kidney is responsible for the excretory function. Its structure is characterized by a well-developed tubular system: the tubules are clearly distinguishable, with defined contours and open lumens. For this reason, any changes — hyperemia, tissue destruction, or loss of structure — should be assessed primarily in relation to the condition of these tubules. Disruption of this architecture underlies the pathological changes observed.
Thus, this image can be considered a morphological baseline, serving as a reference point for the interpretation of pathological findings.
In chronic GBD, fish may survive long enough to reach such stages. Mortality during handling or transfer in these cases reflects pre-existing damage rather than a primary cause.
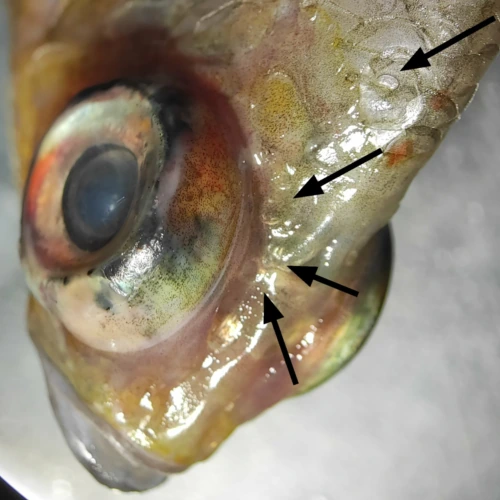
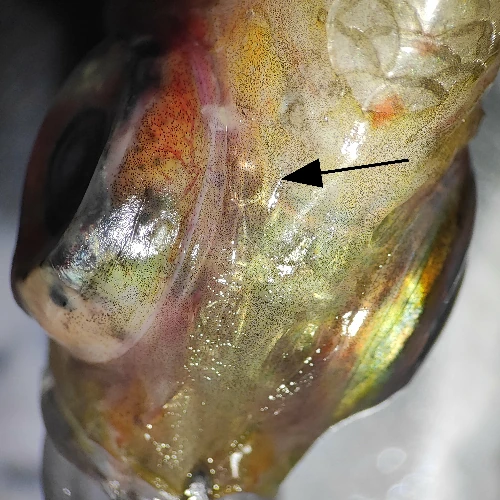
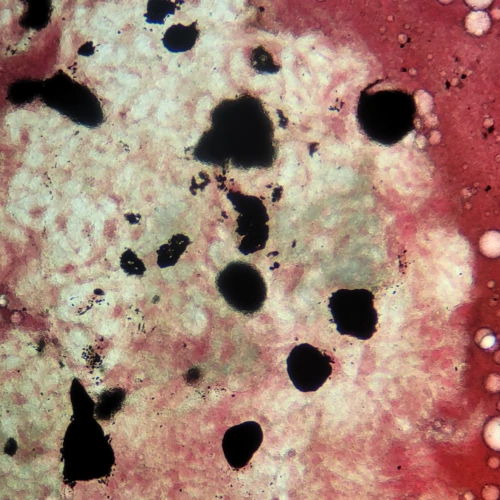
The head kidney is primarily hematopoietic and does not contain renal tubules. However, hyperemia may occur under microcirculatory disturbances. Nearby structures include the eyes, where gas may accumulate depending on species.
Findings include hyperemia, hemorrhages, and gas accumulation.


Gas bubbles may also be observed in the heart, although this is more typical in cases of pronounced supersaturation.

If bubbles are visible in the heart, this may indicate a high level of dissolved gases in the blood. When such blood is transferred with a pipette, gas is released actively and becomes clearly visible. Under normal conditions, blood does not readily form stable foam, and gas release is minimal.
Conclusions
Gas bubble disease cannot be reduced to the presence of bubbles in tissues. It is primarily a disorder of microcirculation and gas exchange that may develop without obvious macroscopic signs. The absence of bubbles at necropsy does not exclude the diagnosis. Conversely, their presence does not confirm it without considering system conditions and clinical history.
The main changes develop gradually and are associated with impaired blood supply. This leads to ischemia, followed by hypoxia and subsequent tissue destruction. The most sensitive organs are the gills, kidney, and brain.
The presence of blood in an organ does not indicate normal function. Vascular engorgement may reflect congestion and impaired outflow rather than adequate circulation. Many necropsy findings require careful interpretation. Gas in tissues may form after death and is not always related to processes occurring during life.
A diagnosis cannot be based on a single sign. It requires integration of morphological findings, environmental conditions, and the history of clinical signs.
Understanding the mechanism is more important than memorizing individual features. Only this allows differentiation between cause and consequence and helps avoid common diagnostic errors.
References
- Hong, W.H., Choi, J.Y., Cho, H.S., Im, J., Park, S.C., Seok, S.H., Kim, S.W., 2024. Gas bubble disease in captive Golden Trevally: Pathological insights and needs for life support system and water quality management. J Aquat Anim Health 36, 348–354. https://doi.org/10.1002/aah.10237
- Pleizier, N., Algera, D., Cooke, S., Brauner, C., 2020. A meta-analysis of gas bubble trauma in fish. Fish and Fisheries 21. https://doi.org/10.1111/faf.12496
- Pleizier, N.K., Brauner, C.J., 2024. Causes and consequences of gas bubble trauma on fish gill function. J Comp Physiol B 194, 739–747. https://doi.org/10.1007/s00360-024-01538-4
FAQ
Is gas in tissues proof of disease?
No. It may form postmortem.
Why do organs appear congested?
Due to blood stagnation, not normal circulation.
Why are bubbles sometimes absent?
Because the process is often subclinical.
Which organs are most affected?
Gills, kidneys, and brain.
Can diagnosis rely on a single sign?
No. Context and multiple findings are required.
See also:
Gas bubble disease. Part I
Gas Bubble Disease: It's Not About the Bubbles
Gas Bubble Disease in fish is not caused by air bubbles entering the gills but by dissolved gas supersaturation. This article explains the …
Granulomas and intracellular agents in fish
 Granulomas and intracellular agents in fish
A collection of real observations: intracellular yeast-like organisms, coccidia, cryptosporidia, and fungal structures in fish.
Granulomas and intracellular agents in fish
A collection of real observations: intracellular yeast-like organisms, coccidia, cryptosporidia, and fungal structures in fish.
Hexamita
 Hexamitids Without Myths
Why hexamitids are not a normal component of fish intestinal microflora, where the myth of 'internal parasites' comes from, and how …
Hexamitids Without Myths
Why hexamitids are not a normal component of fish intestinal microflora, where the myth of 'internal parasites' comes from, and how …
What to do with fish after arrival
 Initial Diagnostics After Fish Transportation
Microscopy, smears, staining methods, and common mistakes in early diagnostics.
Initial Diagnostics After Fish Transportation
Microscopy, smears, staining methods, and common mistakes in early diagnostics.